
ACL Injury Treatment
What is an ACL?
ACL stands for anterior cruciate ligament. It runs diagonally in the middle of the knee. It prevents the tibia (shin bone) from sliding out in front of the femur (thigh bone). It is commonly injured in athletes who participate in sports such as soccer, football, and basketball.
What can cause an ACL injury?
An ACL injury can occur when changing direction rapidly, stopping suddenly, landing from a jump incorrectly or direct contact collision such as a football tackle. Most injuries are complete tears. Partial tears of the ACL are rare but occasionally happen.
What are the symptoms of an ACL injury?
At the time of the injury, you might hear a “popping noise” and you will likely collapse as the knee gives out. The knee will swell within 6 hours and there will be pain especially when weight is put on it. If left untreated, swelling and pain may go away on their own but if your child returns to physical activity the knee will probably be unstable, move abnormally and cause further damage to the menisci and knee cartilage.
What is the treatment for an ACL injury?
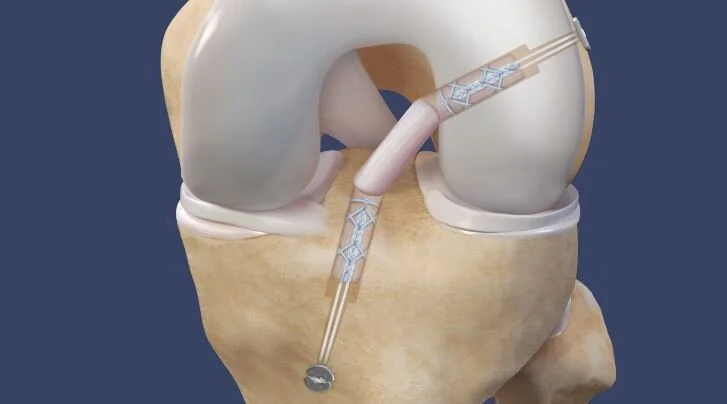
The treatment is called ACL reconstruction. It is a minimally invasive outpatient surgery that reconstructs the ligament using a tissue graft. The provider usually uses quadricep tendons harvested from the same leg that has an ACL tear. Physical therapy is required following surgery to regain motion and strength in the knees.
How long is recovery time?
Recovery time varies from patient to patient. It could take 6 months up to a year to return to full activities. There are very frequent physical therapy visits as well as home exercises for the first three months following the surgery. There are less frequent physical therapy visits for the next three months. Most commonly the injured person returns to sports 9 months after the reconstruction.
Anterior Cruciate Ligament Rupture and Reconstruction:
Ligaments are complex ropes between two bones. They prevent the two connected bones from going too far away from each other. When a ligament is torn and not working two bones at the connected joint can go too far away from each other during normal activities; the joint is “unstable.” The anterior cruciate ligament is the strongest ligament in the knee. After sustaining a tear to it someone’s, knee is usually unstable. She will occasionally feel a strange, painful sensation of her thigh bone hopping abnormally on her shin bone at the knee during a normal action like stepping from a stair or curb. Instability will affect many recreational sports activities. Actions where the athlete plants on the foot of the affected side and cuts toward the opposite direction or when one lands from a jump are affected most. Sheer injuries to cartilage on both sides of the knee bone will result. An ACL deficient knee is far less effective for preventing other serious knee injuries such as meniscus tears than an ACL competent knee is.
ACL ruptures and other serious knee injuries usually result from the knee twisting above a planted foot instead of from violent, high-energy collisions. YouTube has a large number of videos showing athletes at different levels of competition sustaining ACL tears. Most viewers will be surprised to see how subtle the injuries often are.

Girls sustain ACL ruptures far more than boys per hours of sports played. One study found girls are seven times more likely to sustain an ACL rupture than boys. It is common for a patient to concurrently sustain meniscus tears and tears to other ligaments in his knee when he sustains an ACL rupture.

Most young healthy people are going to choose surgical treatment if they sustain an ACL rupture. The surgery is called “ACL reconstruction” and not “ACL repair” because directly sewing the torn ACL together usually does not work. When a ruptured ACL can be directly repaired, The provider directly repairs it. The surgeon views the entire knee with a camera inside the knee (arthroscopy) and addresses other injuries to the knee during the same operation. The torn fibers of the ACL are removed with arthroscopic instruments. The surgeon uses a tendon from the patient or a donor to make the new ACL. The provider uses the patient’s own tendon because an autograft tendon (a tendon removed from the same patient it will be placed in) is less likely to rupture in the future than is an allograft tendon (a tendon from a different person than the patient, generally an organ donor). The provider uses a quadricep tendon as the first choice. The tendon is removed from the same leg as the one having an ACL reconstruction. He uses a suspensory system to place the new ACL.
The patient wears the knee immobilizer except for showers and physical therapy until following up with The provider 3 weeks after the surgery. She will be provided with crutches and will use them to assist weight bearing until it is comfortable to walk without using the crutches. Some patients are comfortable walking without the crutches 4 or 5 days after surgery; some patients need them for more than 2 weeks. Physical Therapy starts ten to 14 days after the surgery; usually before the first follow-up appointment with The provider Physical therapy will require 2 or 3 visits per week until 3 months after surgery. We encourage most patients to start jogging thirty to forty minutes per day 3 or 4 times a week starting 3 months after surgery. No patient is permitted to return to competitive sports earlier than six months after surgery.
There are things that can go wrong during and after ACL surgery. Infrequently, infections inside of the knee or of an incision occur a few weeks after surgery. Post-operative surgical infections are sometimes best treated with a surgery to clean out the infection and antibiotics until all signs of infection are gone. A few patients have a harder time regaining full knee motion after surgery than most patients do. Patients with stiffness will require extra stretching exercises and rarely a manipulation of the knee under anesthesia or arthroscopic lysis of adhesions. Injuries to nerves and blood vessels around the knee have happened during ACL injuries. Some patients have an ACL re-rupture. A re-rupture can happen when they return to play or many years after the surgery. The provider uses a patient’s own tendon instead of a cadaveric one, and does not allow return to full play until more than three months after surgery to help prevent a re-rupture.
Patients are prescribed pain medication to take as needed for a few to ten days after the surgery. Also they are given the handouts and prescriptions below prior to surgery.
These are the list of handouts and prescriptions given prior to ACL surgery: Download ACL Packet
ACL Post-Op Instructions:
You will see you are in a knee immobilizer after waking up, and you need to wear the knee immobilizer except for showers and therapy until you see The provider 3 weeks after surgery.
You can remove the immobilizer and bandages 1-2 days after surgery to bathe. Afterward, you must put the knee immobilizer on but not the bandages. You go home on crutches and can weight-bear as tolerated, meaning that when you are comfortable, you can stop using the crutches. Many patients do well without crutches around one week after the surgery. To minimize school missed due to surgery, some patients are back to school 2 days after the operation and some miss around 2 weeks.
You need to make sure you wear the knee immobilizer correctly, with the patella (kneecap) in the center of the immobilizer.
If you have a problem with receiving your pain medication, please call POBAR from the pharmacy instead of going home and then calling. Calling from the pharmacy will allow us to solve the problem quickly and efficiently.
Answers to Frequently Asked Questions:
The provider does not use hinged knee braces because the knee immobilizer is just as effective in getting patients back to their range of motion, and they are easier and more comfortable to use.
Some doctors recommend CPM machines, however, we do not because it is a hassle after surgery, and often it is painful with no effect on patient outcome.
Knee Immobilizer

Step 1: Feel to make sure the bend in the patient's knee is lined up with the immobilizer. Fold the immobilizer in towards the opposite leg first, followed by the other side.

Step 2: Secure the strap holders on either side of the thigh and use the small straps to hold the foam closed around the leg.

Step 3: Snuggly wrap the straps, starting with the middle.


Finally, place the widest strap diagonally across the patient’s patella (knee cap) after wrapping it tightly. Now you've correctly applied the knee immobilizer!

Follow Us On Instagram!
















Contact us.
If you have any questions or concerns about the services we offer, do not hesitate to reach out by phone or email and a member from our team will follow up with you right away!
appointmentrequests@pobar.org
(813) 548-5056
602 Vonderburg Dr #103, Brandon, FL 33511
This function is used for appointment requests. Unless you’re contacted by the office, your appointment is not confirmed.”